Our Story
...our Journey

PET Scan 1
This is our finial test that is needed before they can diagnose and start treatment for Anthony. PET stands for positron emission tomography. The PET scan uses a mildly radioactive drug that is injected into him. The cancer cells are drawn to this radioactive drug and it will light up the areas where there are cancer cells present.
The doctors want to use this PET Scan to see whether the cancer has spread and they also want to see if the tumor in Anthony’s jaw is the primary source for the cancer.
This test is a huge deal to us, because it will determine if the cancer has spread or not. If the cancer has not spread then Anthony has a 70% survival rate. If it has spread then his survival rate will drop to below 30%. The PET Scan was located in a mobile trailer and Anthony they will need to inject Anthony with the radioactive drug into his arm. This is the 7th shot Anthony has had in the past two-weeks. Anthony was so scared in getting another shot he broke down crying and would not allow for them to give him the shot. After 10-minutes of Anthony crying I had to tell the nurse we need a time out. Anthony and I then exit the building and took a little walk so he can gather his composure. At this point Anthony is just so tired of the pain caused by all of the shots he has had. I told him this is the last test they need to do and just try to be tough and that I’m here with him. We walked back into the room and Anthony still didn’t want the shot. It took a good 10 more minutes before Anthony allowed for him to give him the shot and unfortunately because Anthony was so scared the shot did not take to the vein and they had to poke him once more in order to find the vein.
PET Scan
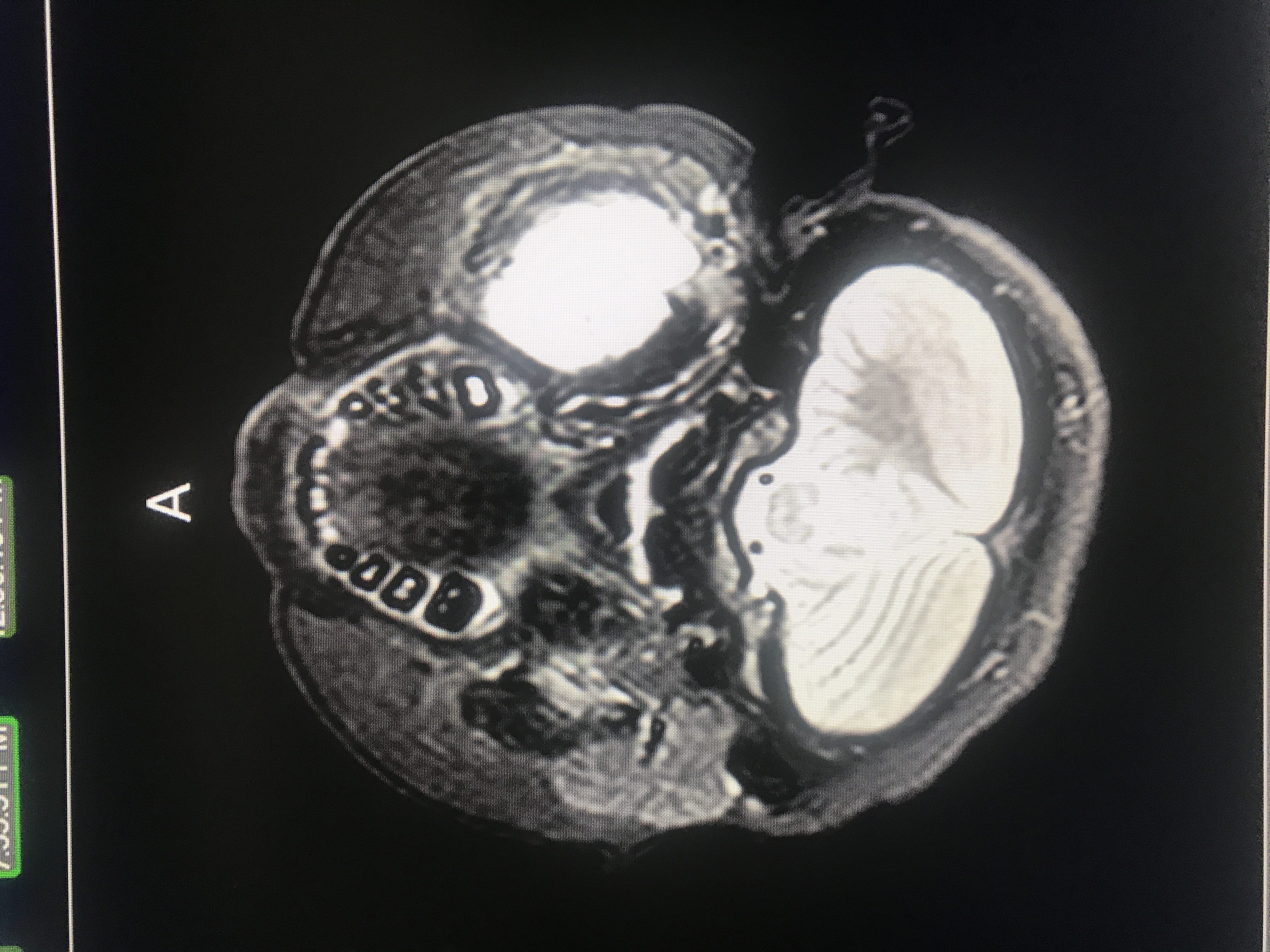
After 30-minuted the radioactive drug has not circulated into Anthony’s system and he can now do the PET Scan. The scan will take around 45-minutes and he will need to stay perfectly still the whole time.
A few days later we got the results. The giant white lump in his jaw is the primary tumor.
We were told that they did not find any metastasis (spreading) of the cancer. This is the best news we could have possibly heard at this time. It seems like since January every news we received was bad news. And the news just kept getting worse and worse every time they told us something. This was truly a break for us and I feel it is a true blessing that his cancer did not spread.
Doctor NOTES:
Pt with newly diagnosed undifferentiated high grade sarcoma left mandible Metastatic work up. CT chest abd pelvis negative, PET scan primary is avid and localized, bilateral bone marrow negative. Left mandible has been noted to be swollen for over 2 months, CT scan 2/16 abnormal, bx early march, pathology sent to CHLA
MRI 3/16:5.6 x 5.1 x 3.0 cm CC by AP by transverse. There is internal areas of nonenhancement, likely reflecting central cystic changes, and/or necrosis. There is posterior displacement of the left parotid gland, and displacement of the muscles of mastication. There is left level I be lymph nodes up to 1.5 x 1.0 cm, and left level II nodes up to 1.7 x 1.1 cm.
Oncokids NGS pending
PFHx: No cancer history, no medical problems
Review of Systems
Constitutional: Negative for chills, fever and weight loss.
HENT: Negative for nosebleeds.
Respiratory: Negative for cough and hemoptysis.
Gastrointestinal: Negative for blood in stool.
Genitourinary: Negative for hematuria.
Endo/Heme/Allergies: Does not bruise/bleed easily.
SARCOMA
Note:
Undifferentiated sarcoma > 5 cm localized
Discussed with surgeon (McNichol) who feels that tumor is completely resectable and it would be reasonable to operate before or after chemo. However in the pandemic environment prefer to delay long complicated surgery until after the surgery.
Will model ARST0332 arm D
4 cycles of chemo before surgical resection with Ifosfamide, Doxo and Zinecard as Cardioprotectant
Discussed Dx of malignancy with patient and family. Discussed that a malignancy is caused by over growth of a particular cell related to a genetic mistake within the tumor that we may or may not be able to identify. I explained that although there may be environmental risk factors at this time we are unable to identify specific causes of the malignancy. I reassured the family that there was nothing that they could have done to cause or prevent this cancer from developing.
We discussed the use of chemotherapy to treat malignancies and the general side effects of chemotherapy including hair loss, nausea and vomiting, risk of sterility, bone marrow suppression including the need for transfusion of red blood cells and platelets. We discussed the use of clinical research in designing treatment plans for children with malignancies, our participation in the children’s oncology group and the concept of participation in clinical trials if there is a specific trial opened for his disease.
Next Article - PICC Line